Author: Héctor Hugo Escutia-Cuevas MD1*
1 Interventional Cardiology, Regional Hospital ISSSTE Puebla, Puebla City, Mexico.
Introduction
Chronic total occlusion (CTO) represents the most challenging setting for percutaneous coronary intervention (PCI) and multivessel coronary disease (MCD) is often treated in a staggered manner and in a deferred procedure. Although transfemoral is one of the common access site, the transradial access (TRA) has been used with similar procedural success[1].
The distal transradial access (dTRA) as default approach for coronary angiography (CAG) and interventions is also used in Latin-America. This technique has many advantages in terms of enhancing patient comfort, reducing access-site bleeding, faster hemostasis, and diminishing radial artery occlusion[2]. The MCD can be treated by PCI when the patient has the necessary conditions, does not suffer from diabetes and the treatment is carried out in a single procedure when there is hemodynamic stability and the use of contrast has been minimal. Although dTRA has shown clinical advantages, when performing dTRA in CTO cases, there are concerns about its safety and efficacy because of higher procedure complexity and the need for strong guide catheter support[1]. In such case, thin-wall sheath with good kink resistance and large inner lumen would be crucial to perform CTO cases via dTRA access.
A clinical case is shared in this article to discuss the role of sheath plays regarding treating CTO cases via dTRA access and maintain the clinical benefits at the same time.
Case Sharing
A 75-year-old man with hypertension, chest pain at minimal effort, and ischemia detected with dobutamine-stress echo was referred to CAG, which showed proximal right coronary artery (RCA) CTO (J-CTO 2 points), with strong Rentrop 3 collaterals from the anterior descendant artery (ADA). Likewise, ADA is evidenced with diffuse disease and severe angiographic calcification and focal disease in a Posteriorlateral (PL) branch. After consensual decision by the patient and the heart team (SYNTAX score 23 points, SYNTAX II PCI 4 year mortality 5.7%), it was decided to perform PCI. Two days after the baseline CAG, the procedure was done via bilateral dTRA, with two 7Fr radial sheaths (Braidin™, APT Medical, Shenzhen) for dual coronary injection (Figure 1A-D).
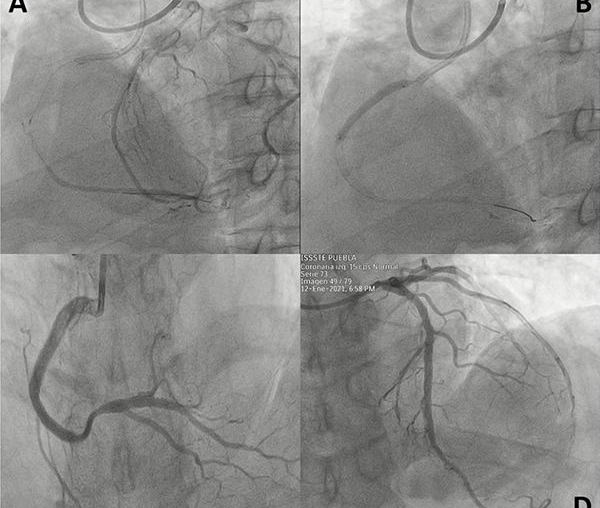
By antegrade wire escalation and balloon predilations, the RCA was successfully recanalized, with a 4.0 x 38 mm everolimus-eluting stent carefully and optimally deployed at its ostialproximal segment. As the necessary conditions of stability existed after CTO-PCI, PCI is performed at the ADA with two everolimus-eluting stents (3.5x24mm and 3.0x28mm) with a residual iFR of 0.93. The PL branch, having a type A lesion, was treated conventionally with a 2.5x24mm everolimus-eluting stent (Figure 2A-D). With a total procedure time of 60 minutes and 150ml of contrast used.
Adequate hemostasis was obtained after 2 hours of continuous adapted pneumatic bands, without any bleeding. Bilateral proximal and distal radial pulses were easily palpable after hemostasis and at hospital discharge the next morning, without any minor or major accesssite or clinical complications. Bilateral dTRA for complex CTO-PCI by experienced transradial operators is feasible and safe, MCD treated by PCI can be carried out in a nonstaggered manner when the necessary conditions exist in the procedure and patient safety is not affected.
Discussion
Studies shown that dTRA could be a preferred approach as it could bring certain clinical advantages. For example, enhancing the patient’s comfortability given with a rest palm position[3]; shortening the time of hemostasis compression[4]; protect the arteriovenous hemodialysis access for chronic kidney disease patients; reserve the radial access site for future CABG or intervention procedures etc.
Traditionally, 6F introducer is used commonly in coronary percutaneous intervention. The use of larger French size introducer like 7Fr would be challenging in dTRA especially for CTO cases. Sometimes have to compromise and choose to use a smaller French size introducer because large sheaths outer diameter and small radial artery could be the risk factors for developing radial artery occlusion or other complications[5]. To solve this, study finds that downsizing coronary interventional material and equipment, such as thin-walled equipment, is suggested to reduce bleeding complications, hemostasis time and rates of radial occlusion[6]. In the case shared above, 7Fr Braidin™ thin-walled introducer sheaths (APT Medical, Shenzhen) were used as the solution bilaterally. The introducer is made of braided thin-wall, it is designed to provide good kink resistance and accomplish the dTRA without compromising the inner lumen French size. The sheath also contains hydrophilic coating and study find that radial spasm could be reduced after using a hydrophilic coated sheath[6]. With the use of a thin-walled introducer, the PCI was performed successfully in the CTO case without access site complications.
However, studies also shown that there are some cautions when using dTRA. In common, puncture time via dTRA would be longer than traditional radial approach and the artery vessels could be more curved, which may increase the difficulty of facilitating the guide wire[7-8].
Conclusion
With the use of suitable tools, dTRA is achievable and safe in CTO cases, meanwhile obtaining the clinical benefits such as reducing chance of complications and enhancing the patient comfort. A thin-walled introducer sheath would be the first step of successful PCI and CAG. With the new options of thin-walled introducer, dTRA could be more feasible in CTO cases in the usual practices.
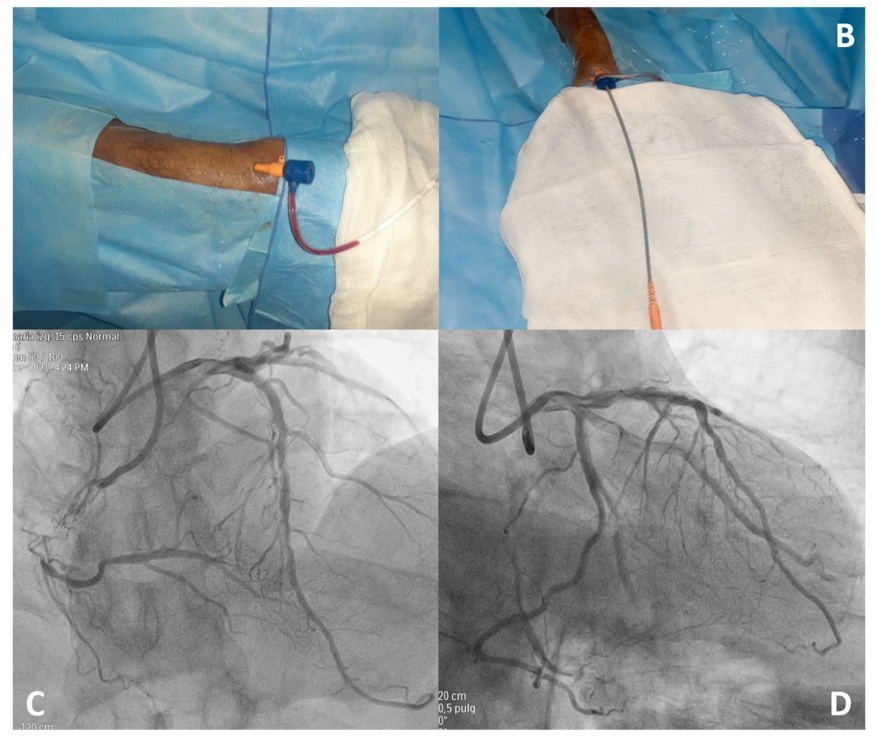
Figura 1.- A) Acceso transradial distal derecho. B) Acceso transradial distal izquierdo. Ambos introductores radiales de 7Fr (APT Medical, Shenzhen, China) para inyección coronaria dual. C) Angiografía coronaria que muestra OTC de arteria coronaria derecha proximal (J-CTO 2 points), y arteria descendente anterior con enfermedad difusa con calcificación angiográfica severa (D).
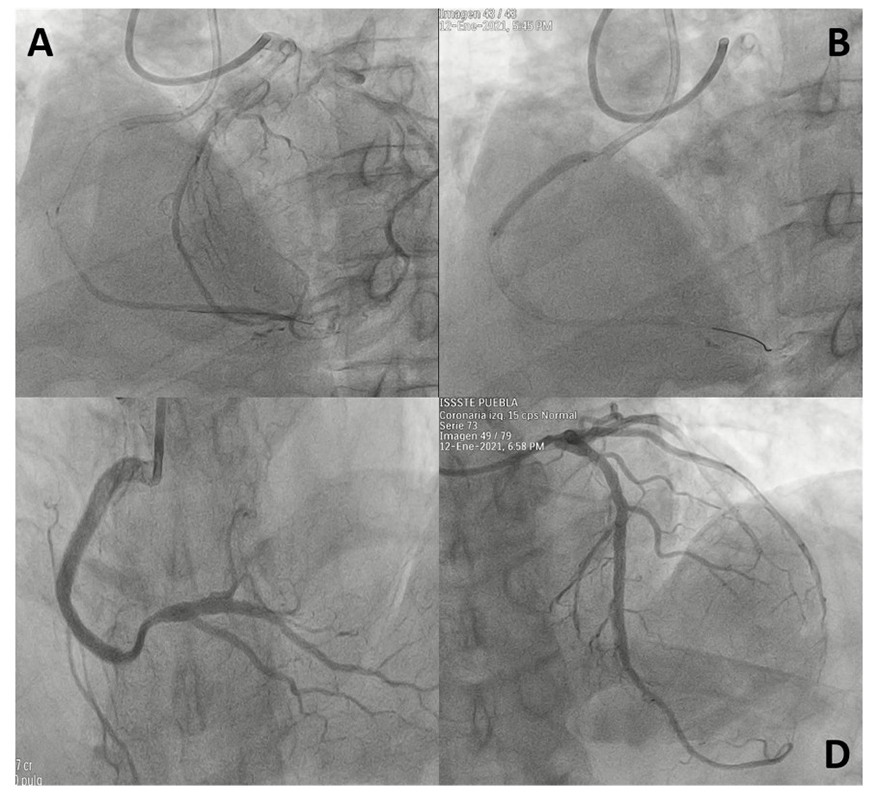
Figure 2.- CTO PCI and MVD PCI. Successful Anterograde Wire Escalation crossing through the CTO in 10 minutes (A), with everolimus-eluting stent implanted in the proximal segment of right coronary antery (B). Final angiographic result of right coronary artery PCI (C). Final angiographic result of anterior descendant artery PCI.
References
1. Megaly M, Karatasakis A, Abraham B, Jensen J, Saad M, Omer M, Elbadawi A, Sandoval Y, Shishehbor MH, Banerjee S, Alaswad K. Radial versus femoral access
in chronic total occlusion percutaneous coronary intervention: a systematic review and meta-analysis. Circulation: Cardiovascular Interventions. 2019 Jun;12(6):e007778.
2. Mason PJ, Shah B, Tamis-Holland JE, Bittl JA, Cohen MG, Safirstein J, Drachman DE, Valle JA, Rhodes D, Gilchrist IC, American Heart Association Interventional
Cardiovascular Care Committee of the Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing; Council on Peripheral Vascular Disease; and
Council on Genomic and Precision Medicine. An update on radial artery access and best practices for transradial coronary angiography and intervention in acute
coronary syndrome: a scientific statement from the American Heart Association. Circulation: Cardiovascular Interventions. 2018 Sep;11(9):e000035.
3. Gasparini GL, Garbo R, Gagnor A, Oreglia J, Mazzarotto P. First prospective multicentre experience with left distal transradial approach for coronary chronic
total occlusion interventions using a 7 Fr Glidesheath Slender. EuroIntervention: journal of EuroPCR in collaboration with the Working Group on Interventional
Cardiology of the European Society of Cardiology. 2019 May 20;15(1):126-8.
4. Aoi S, Htun WW, Freeo S, Lee S, Kyaw H, Alfaro V, Coppola J, Pancholy S, Kwan T. Distal transradial artery access in the anatomical snuffbox for coronary
angiography as an alternative access site for faster hemostasis. Catheterization and Cardiovascular Interventions. 2019 Nov 1;94(5):651-7
5. Aamir S, Mohammed S, Sudhir R. Transradial approach for coronary procedures in the elderly population. Journal of geriatric cardiology: JGC. 2016 Sep;13(9):798.
6. Rathore S, Stables RH, Pauriah M, Hakeem A, Mills JD, Palmer ND, Perry RA, Morris JL. Impact of length and hydrophilic coating of the introducer sheath on
radial artery spasm during transradial coronary intervention: a randomized study. JACC: Cardiovascular Interventions. 2010 May;3(5):475-83.
7. Vefalı V, Sarıçam E. The comparison of traditional radial access and novel distal radial access for cardiac catheterization. Cardiovascular Revascularization
Medicine. 2020 Apr 1;21(4):496-500.
8. Koutouzis M, Kontopodis E, Tassopoulos A, Tsiafoutis I, Katsanou K, Rigatou A, Didagelos M, Andreou K, Lazaris E, Oikonomidis N, Maniotis C. Distal versus
traditional radial approach for coronary angiography. Cardiovascular Revascularization Medicine. 2019 Aug 1;20(8):678-80.